Key takeaways from the study
This paper examined whether topical tretinoin, a retinoid long used in dermatology, could promote hair growth in people with androgenetic alopecia, either on its own or combined with a low concentration of topical minoxidil. The researchers followed 56 adults over several months to more than a year, using hair counts and photographs to track changes in a defined scalp area.
They found that tretinoin alone led to some degree of hair regrowth in about 58 percent of participants, usually modest. When tretinoin was combined with 0.5 percent minoxidil, 66 percent of participants showed increased terminal hair growth, with nearly half classified as having a strong response. Minoxidil at this low dose, when used alone, did not produce meaningful regrowth.
Why this matters is not that tretinoin suddenly becomes a stand-alone solution for hair loss, but that it appears to influence the biology of the hair follicle and the surrounding skin. The authors suggest it may stimulate cell turnover, affect blood vessel growth, and increase the penetration of other topical agents.
The limitations are substantial. These were small pilot studies, not large randomized trials. Responses varied widely, and results took many months. The findings point toward possibility and mechanism, not proof or prescription.
The context and purpose of the research
In the early 1980s, treatment options for pattern hair loss were limited and inconsistent. Minoxidil was gaining attention, but even at higher concentrations it helped only a portion of users, and often produced fine, fragile hairs rather than durable regrowth. At the same time, dermatologists were deeply familiar with tretinoin as a treatment for acne and photoaged skin. It was known to change how skin cells grow, divide, and mature.
Clinicians also noticed something unexpected. Some patients treated with retinoids, including isotretinoin for acne, developed increased fine hair growth on the face or scalp. These observations were not planned outcomes, but they raised a reasonable question. If retinoids can alter epithelial behavior so profoundly, could they also influence hair follicles, which are specialized skin structures?
The purpose of this research was exploratory. The authors were not trying to establish a new standard therapy. They wanted to test whether topical tretinoin had any measurable effect on hair growth, and whether it might enhance the effects of minoxidil when the two were used together. The work reflects a period when careful clinical observation often preceded formal large-scale trials.
How the research was conducted
The study included 56 adults between 20 and 64 years old, all diagnosed clinically with androgenetic alopecia. Participants were divided into small groups receiving different topical treatments applied twice daily to affected scalp areas:
- Tretinoin 0.025 percent alone
- Minoxidil 0.5 percent alone
- A combination of tretinoin 0.025 percent and minoxidil 0.5 percent
- A vehicle solution serving as placebo
To track changes consistently, investigators selected a one-inch circular target area on each participant’s scalp. They counted terminal hairs within that area at baseline and during follow-up visits, using defined landmarks to ensure accuracy. Photographs were taken before and during treatment to visually document changes.
Participants were monitored for skin irritation and general health measures such as blood pressure and laboratory values. Follow-up lasted from several months up to 18 months, reflecting the slow pace of the hair growth cycle.
Results observed in the study
The researchers categorized outcomes based on the percentage increase in terminal hair count within the target area.
- Participants using placebo showed no meaningful hair growth.
- Those using 0.5 percent minoxidil alone did not show terminal hair regrowth, although one developed fine vellus hairs.
- Among participants using tretinoin alone, about 58 percent experienced some regrowth, usually modest and often involving finer hairs.
- In the combination group, 66 percent showed positive responses. Forty-four percent were classified as having a strong response, while 22 percent had a moderate response.
One striking case involved a woman with more than 20 years of pronounced androgenetic alopecia who experienced substantial regrowth over 18 months using tretinoin alone. Other cases showed gradual filling in of frontal or vertex areas after months of combined therapy.
Image placeholder


Source: Bazzano et al., Journal of the American Academy of Dermatology, 1986, Figure 1
9 months of combination therapy with tretinoin and minoxidil.
Source: Bazzano et al., Journal of the American Academy of Dermatology, 1986, Figure 2
combination therapy with tretinoin and minoxidil. Top, Before treatment. Bottom,
After treatment.
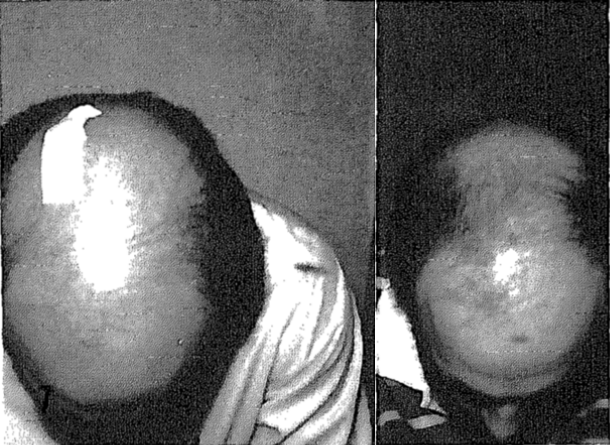
Source: Bazzano et al., Journal of the American Academy of Dermatology, 1986, Figure 5

combination treatment with tretinoin and minoxidil. Left, Before treatment. Right,
After treatment.
Source: Bazzano et al., Journal of the American Academy of Dermatology, 1986, Figure 6
therapy with tretinoin and minoxidil. Note new hair growth advancing from parietal
area toward crown. Left, Before treatment. Right, After treatment.
Source: Bazzano et al., Journal of the American Academy of Dermatology, 1986, Figure 7
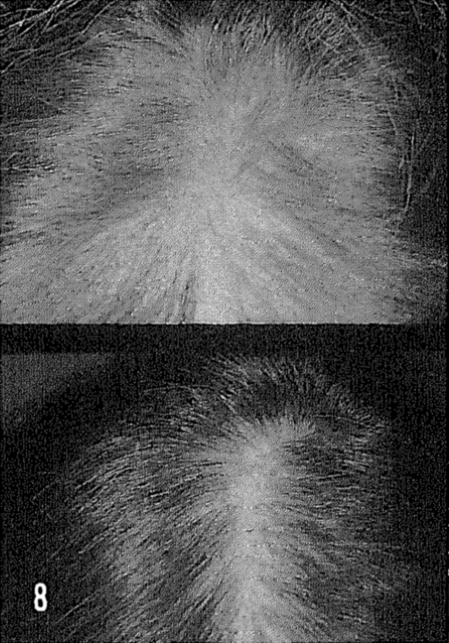
to retinoic acid-only therapy (tretinoin). Response occurred within 1 year of therapy. Top, Before
therapy. Bottom, After therapy.
Source: Bazzano et al., Journal of the American Academy of Dermatology, 1986, Figure 8
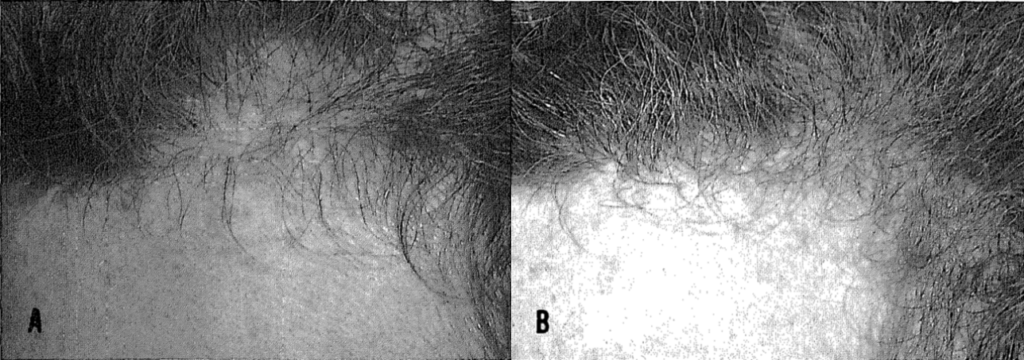
frontal area filled in after 6 months of retinoic acid treatment. A, Before treatment. B,
After treatment.
What the conclusions show, and what they do not
From these results, the authors concluded that tretinoin appears to influence hair growth when applied topically, and that it may act synergistically with minoxidil. In simple terms, tretinoin seems to prepare the scalp and follicle environment in a way that allows other growth-promoting signals to work more effectively.
What the study shows is that hair follicles, even in androgenetic alopecia, are not always biologically inert. Some retain the capacity to respond to changes in their cellular environment. Retinoids may play a role by increasing cell turnover, influencing differentiation within the follicle, and possibly supporting local blood vessel growth.
What the study does not prove is equally important. It does not establish tretinoin as a reliable or sufficient treatment on its own. It does not guarantee results, durability, or safety for all users. And it does not replace the need for larger, controlled studies. The findings are suggestive, not definitive, and should be understood as a step toward understanding mechanisms rather than a final answer.
Relevance to topical approaches for alopecia
This research is directly related to topical treatments for hair loss because it shifts attention from single active ingredients to the condition of the scalp and follicle environment. Tretinoin is not primarily a hair growth drug. Its main effects are on skin biology.
The study suggests that improving how the scalp renews itself and how substances penetrate the skin may influence hair outcomes. In this sense, tretinoin functions less as a growth trigger and more as a facilitator. It may help other topical agents reach their target more effectively and may create conditions that support follicle activity.
For topical approaches to alopecia, the implication is that combination strategies and supportive agents deserve attention. Hair growth may depend not only on stimulating follicles, but also on restoring a healthier, more responsive scalp environment.
Who this study matters most for
This study matters most for individuals who are curious about why topical treatments work for some people and not for others. It offers cautious encouragement to those with early to moderate androgenetic alopecia, where follicles may still retain responsiveness.
It may also resonate with people who have tried single-agent topical treatments without meaningful results and wonder whether the issue lies in absorption, scalp health, or follicle signaling rather than in the active ingredient itself.
For clinicians, researchers, and informed readers, the study provides a framework for thinking about hair loss as a problem of tissue biology, not just hormone sensitivity. It suggests that even long-standing conditions may contain pockets of reversibility, given the right local conditions.
Sources and citations
Primary study
Bazzano GS, Terezakis N, Galen W. Topical tretinoin for hair growth promotion. Journal of the American Academy of Dermatology. 1986;15:880–883.
Selected references cited by the authors
Olsen EA et al. Topical minoxidil in early male pattern baldness. Journal of the American Academy of Dermatology, 1984.
DeVillez RL. Topical minoxidil therapy in hereditary androgenetic alopecia. Archives of Dermatology, 1985.
Sundelin J et al. Structure and tissue distribution of retinoic acid binding proteins. Journal of Investigative Dermatology, 1983.